In this webinar, hear from two senior living organizations who have successfully adopted infection control technology at their organizations.
Listen and learn:
- Best practices implementing infection control management software
- How did these solutions impact their teams?
-How did they manage unwelcome visitors like influenza, norovirus and C.diff?
Are you ready to improve infection control at your community?

Webinar transcript:
Mark Anderson:
Hello everyone and welcome to today's Leadership Forum webinar series. Appreciate you joining us today for this month's webinar. I'm your host, Mark Anderson, chief client officer here at Eldermark. My contact information is there. Feel free to contact me at any time about your ideas for these webinars or anything you'd like us to talk about on these webinars or just anything else that we can do to help you hear from Eldermark. For those of you that may be new to this series, a little bit about this webinar series, they are intended to connect us all as leaders in senior living to learn, share and support each other in our work. So if this is your first time attending one of these webinars, I hope you will have a good experience today and that we will be able to see you again at future webinars. Just a couple housekeeping reminders for our customers, if you have any key staff changes going on at your community or your organization, please let us know at support@eldermark.com so we can keep our records up to date.
And then be sure to read the stuff that we send you, especially our latest release notes. And we are also sending out a newsletter now periodically, so watch for that. There's some actually really good content in there. And again, the stuff that we send out is truly meant to keep you up to date and to make sure that you are aware of stuff going on here that may affect not only how you use our stuff, but how you do your job. Just a couple updates before we begin our webinar topic. Just wanted to plug a couple newer things going on here at Eldermark. Firstly, ElderSmarts, this is our new analytics as a service data management system.
We're having a lot of fun with this with our current ElderSmarts customers, putting together some prescriptive and predictive analytics, pulling together data from their systems to give them the analytics that help inform them as they work to achieve their goals. Some of the content sets that we have built in the analytics for our customers include topics such as resident acuity, staffing, of course financial performance, occupancy, quality indicators and more. So if you want to learn more about ElderSmarts, let me know or let your account manager know or any of us here at Eldermark and we can connect you with some additional information. And then secondly, ElderForms. This is our newer electronic document management solution. We do this in concert with Worldview Technology Solutions, a sister software company. Basically what ElderForms does is it manages all of your forms electronically, including the obtaining of signatures, either in person with a stylus or the finger on a touch screen, or sending those forms and documents to a resident responsible party for review and signature and return.
And ElderForms does also include kind of a ElderCharts electronic file management system as well. It's really taking off. You want to learn more about that? Let one of us know here at Eldermark and we'll connect you with the right folks. Okay, just a few notes before we begin our presentation and introduce our guest and her guests today. All of you will remain muted during the webinar today. If you have a question for any of us, please use the question feature on the webinar control panel and we'll get to your questions as time permits. Generally, we are able to get to all the questions, so don't be shy about asking something that you would like to know. You will receive a link to the recording of this webinar within about 24 hours after we adjourn the webinar today. So that'll come to you in your email as a registrant.
And again, you're welcome to contact our presenters or myself at any time directly via email. Please do so with any of your questions or comments. Happy to address those for you. All right, so moving on. Our topic today is around infection control. Don't sweep your infections under the R.U.G.S. Our guest speaker will explain what is meant by that. We've come a long way in infection control and senior living. I remember back in the day as a former operator, and even when I started working in this business way back in high school, that was a long time ago, infection control for us was really mostly centered around hand washing. It wasn't very often that we went beyond that other than you just keep a good clean facility and you make sure that your residents enjoy good hygiene. And again, it was mainly hand washing. And then, you fast forward now to today and the landscape has really changed for the senior living operator around infection control practices.
Certainly the demands for these practices are increasing. So our caregivers, they really need good methods to help manage infection control practices, especially with increasing regulatory compliance demands. For example, now here in Minnesota over the last couple of years, the regulations are such that in this state, and I understand in some others, that assisted living communities are required to follow the same infection control guidelines as skilled nursing facilities. And they are then surveyed accordingly, not only by state health authority, but also by state OSHA authority. And then I thought this was a really telling statistic to kind of introduce and set the stage before we get into our presentation.
And a third of all deaths in people over the age of 65 can somehow be linked to infectious diseases. And with weaker immune systems among older adults, they can become more susceptible to an infection when they become sick or inflicted with some other type of disease process. And so, good infection control practices can indeed reduce hospitalizations, certainly transition events, and most importantly save lives. So with that, I would like to introduce our guest presenter, Christina Haeg. Christina is the client solutions director at Peerlytics Infection Control Management software solution. And so I am going to turn things over to Christina because Christina also has a couple of guests to help her tell her stories today. So Christina, take it away.
We're going to give Christina a moment to grab the screen. Christina's a little frozen this afternoon, so we'll give her an extra minute. She is offsite at a conference, so there we go. I can't hear you yet, Christina, but you may have to stay off camera to keep your bandwidth strong. Sorry for the delay. We'll give Christina an extra minute. Her internet is not that strong where she's at. How are we doing, Christina? We still can't hear you. So sorry for the delay. While we're waiting for Christina to connect, I might be able to fill in here. Just a moment. I think we may have lost Christina completely.
Well, I tell you what, while Christina is working to get reconnected, I am going to introduce a couple folks that have agreed to join us this afternoon. And to talk about their experience in infection control management using technology, we thought it would be of great help to bring on some providers, a clinician and an administrative physician representative to kind of share with us their experience in moving from other systems and managing infection control to using some type of software. So I'm wondering if I could get Michelle and Angie to turn on their cameras and join us here in the presentation. There's Angie. And Michelle, we'll watch for you. There's Michelle. Hello. How are you guys? While we wait for poor Christina, I don't know where she's at. I want to.-
Christina Haeg:
Okay. Can you guys hear me?
Mark Anderson:
Well, now we can.
Michelle Ehrenberg:
Welcome back.
Christina Haeg:
Oh my goodness.
Mark Anderson:
We lost you for several minutes, so we've been improvising. I was just ready to introduce Angie and Michelle, but if your audio is back, you can start over and introduce these guys and how they're going to help tell our story today.
Christina Haeg:
Okay, excellent. And am I sharing my screen?
Mark Anderson:
You are. We are on, yeah, the impact screen.
Christina Haeg:
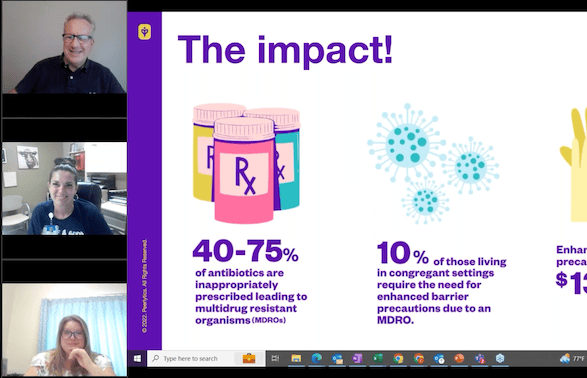
Okay. Okay. It's like no matter how much we practiced and prepared, here we are. Right? So thank you so much to Angie and Michelle and sorry for the technical difficulties here. But I am super excited to have these two on to share their wealth of knowledge that they bring to this topic. Michelle comes to us with administrative or administrator background, and we're going to get to some Q&A from her. And Angie comes with the clinical lens with nearly 20 years of nursing experience, and she's excited to share her passion about infection prevention too. So let's breeze through some of these slides and then we'll get to this Q&A piece. And as I had said, but you did not hear me, but setting the stage to the impact that infection prevention has and infection management has pairing up with the staggering statistic that Mark shared about the number of those impacted by infections, it's really important to understand where we're at, the dollars that are being spent in inefficient practices and workflows, especially when we look at our residents in senior living and those living in skilled nursing.
So 40 to 75% of the antibiotics are inappropriately prescribed leading to multi-drug resistant organisms. So these are things like C.Diff, VRE. 10% of those that live in congregate settings require the need for enhanced barrier precautions due to these MDROs. So this is the need for masking, gowns that our caregivers would be needing to don and doff to keep other residents and themselves safe. And this then results in about $13 a day per resident to maintain this type of PPE use. Antibiotic related infection management is resulting in about 23 hours a month that nurses and front end staff are needing to manage to call the pharmacy, get the medication, get the med into the resident's hands and so forth.
So, it's a pretty substantial amount of time. The dollars in lost revenue here due to potential hospitalization is about $200 a day. And those that have had Mark share his story, and maybe Mark you plan to share that study later on too, but this is a pretty staggering number that this is potential loss revenue from a leave of absence or a hospitalization. And communities are spending about $2,500 a month in infection related expenses. And I think the most important metric to capture on this screen is that half of these healthcare acquired infections and quite possibly more are avoidable and preventable. So that's what we're going to talk a little bit more about.
Mark Anderson:
Well, and I can add some other dollars to that slide. Christina, you mentioned the study that I did, so I'll just plug it in here because it fits right in there. And that is, a few years back, I did a study on leave of absences in senior living. And we studied four customer organizations. It came to about 2,900 resident health records that we studied. And I looked at all the clinical related leaves of absence, the reasons for those, how long they were and so on, and contributing factors and all that because the idea was, what can we do to better affect these leave of absence events so that we can better mitigate or even prevent them? Well, one of the things we learned in putting a dollar value to these is that, first of all, the average length of time away from the community was almost 13 days across all clinical related leaves of absence.
And interestingly, that was about the same amount of time that residents were spending in a typical transitional care unit admission, which helped fortify our data. But the lost service revenue for each of those leave of absence events was 12 to $1,500 per event of loss service revenue across the organizations that were in this study. And we looked at data over a year. It was not far from $2 million in lost service revenue across those four organizations, those 2,900 resident records. So it really did represent a financial impact on the communities and gave rise to interest in finding ways that we could do better in our care management systems to better mitigate or prevent those transition events. Which gets to your work, Christina, in what Peerlytics can do in helping and what technology can do in helping the clinician with better management systems for infection control practice.
Christina Haeg:
Absolutely. And I think in the next few slides here, I'm hopeful that attendees will learn some key takeaways and things that they could implement very easily today to be able to start seeing some impacts on how care is being delivered, especially in terms of infection management. So those that have heard me speak before know I feel very passionately about prioritizing people over paper. And so much of what we have seen in healthcare and it continues to transpire as Mark had alluded to prior is compliance regulations coming from state governing bodies. And so much of what we do is kind of guided in these regulations by OSHA as well. But if we can use evidence-based practices and we keep our team members top of mind and our residents top of mind, we're going to be compliant using those tactics. And so when we prioritize people over paper, when we look at our processes and our workflows and kind of step away from the compliance piece, especially in terms of spreadsheets and managing and tracking things that way,. We can still be compliant and avoid fines.
We can preserve our resources when we think about the slim workforce that we have now. And if we're not tracking our staff illnesses effectively, quite possibly we could be getting other residents sick that's going to take more resources from our frontline workers to care for those residents during an already slimmed workforce. Or if we're not tracking our staff illnesses and understanding what's happening with our resident illnesses, are there correlations, are there precautions that we can put in place to avoid this from spreading to continue to preserve our resources? And then, in doing so, we're going to improve resident outcomes, we're going to improve care and we're going to see some better staff satisfaction in being able to work in an environment that's not getting ourselves sick, getting our families sick when we are using precautions and we're able to be able to see these trends and put things in place.
So all around some really great things if we just step back and look at evidence-based best practices, back to the basics we've all heard, right? Going back to the hand hygiene piece of it. Doing all those things is going to keep us compliant. So some infection management best practices when we look at how to track trend infections and infection control is such a huge topic and really one that's been, the tapes have been played well for the last three years. But really what I want to kind of focus on today and what our panelists will bring in is some additional feedback to this. But we really need things to be rooted in real time. We need to be monitoring symptoms, and that's where this R.U.G.S. piece is going to come into play. We need to be spreading our workload beyond our clinical department. So this should not fall on one nurse in a senior living community to make sure that they're the only one that has infection prevention top of mind. We really need to be spreading this workload beyond the clinical team. We need to have up-to-date staff call-in data collection.
Why are our team members calling in when they're ill? What locations have they worked primarily within the last 72 hours and what department? And when we track these things efficiently, we're able to see some trends, and like I said, put some precautions in place to avoid a spreading of an illness. And then we need continuous training on infection prevention measures. And this includes auditing the success of our training. How do you know that your team members are washing their hands after performing cares? How do you know that your team members are putting on PPE appropriately for the right level of precaution? And this isn't a one and done type event. This isn't training our team members on proper hand washing. This is continual education to continually keep infection prevention top of mind.
So R.U.G.S came to be when we stepped back and looked at the four buckets, I'll say, of illnesses, types of illnesses that show up with our population, and that's respiratory, urinary, gastro and skin. And I really like this kind of concept and thought that, when you keep sweeping things under the rug, eventually you're going to trip from the mess you've made. And that really comes back to, if we're not tracking these things, if we're not getting our frontline caregivers or our dietary team members out in the dining room empowerment to be able to bring these signs and symptoms forward of our residents, things are going to get missed.
And the acuity that that resident exhibited at eight in the morning could be a full blown crisis situation and result in a hospitalization 12 hours from there. So this was a condensed way, an acronym if you will, to say, how can we make this easy for those folks that aren't clinical, but to be able to say R.U.G.S? Keep R.U.G.S top of mind when you're working with residents, when you're passing people in the hallway. Are any of these symptoms being noticed? And can you bring those forth to your clinical team in hopes to get the assessment and the care that this resident needs sooner before there is a crisis?
So making infection prevention everyone's intention comes with workflows, right? Slimming things down, simplifying things and being able to repeat the cycle in education and understand your gaps. So part of that is what I just talked about. Symptom identification. Getting everyone working in your community to understand this kind of R.U.G.S mentality, being able to be attuned to maybe some acute changes within residents, being able to self-report any of those symptoms under that R.U.G.S acronym that they may be experiencing, knowing that those could be passed on to residents or to other team members. So symptom identification is first here, then there's the clinical piece of it. So getting that clinical assessment, getting that tracking down, being able to document these changes. What happened as a result of the runny nose, the cough, the sore throat? What happened as a result of the comfort with going to the bathroom or documenting those things so that we can be able to note those changes and get our patients the right care at the right time.
But then, nope, I got to get my mouse there. Converting that data into knowledge. So using a system, say it be a spreadsheet, say it be a software solution that allows you to take all of that information and convert some of that data into knowledge to understand your gaps, to see where did this infection trend start, where did it go, what did we learn from it? Understanding your patient's history. Are we continuing to get a UAUC when our resident is exhibiting these symptoms, when we're treating a colonized UTI, for example?
But if we're not tracking and charting and documenting those things, we're not going to be able to see those trends and we could be spending a lot of time doing a clinical pathway that really isn't appropriate. So converting data into knowledge. And then, the last piece in this is educate and audit based on the gaps. So what did your data tell you? What education can you get in front of your team members so that each of these pieces can be more succinct and help streamline this workflow which we know will maximize dollars in our community, keep our residents safe and keep us compliant.
So, super excited for Michelle and Angie to be here. Michelle brings 25 years of experience from the industry and overseas operations at Minnewaska Community Health Services, which includes four skilled nursing facilities. It was a fun fact to learn about you, Michelle, that you are an EMT and that you volunteered your time on the ambulance. That's fantastic. I did not know that. So given your experience and given your operational experience, I really just kind of want to pick your brain while we're here and see, you have used other infection tracking softwares before. What led you from kind of migrating things off of paper and out of Excel?
Michelle Ehrenberg:
Right, so we've actually used a couple internet based infection control softwares as well. The thing that stuck out to us the most about Peerlytics is the quantitative and the qualitative data, being able to bring that all into one and knowing that it's coming from everywhere. You're not looking at a spreadsheet or emailing somebody. You're able to open up the program and see, okay, we've had two staff members that have been out with stomachaches for the last two days. The last time they worked, they were on the north wing of the nursing home. Oh goodness, we have an individual down there that may have an issue now. All right, this is time to educate, this is time to ensure that we are combating whatever we can infection wise to prevent this from going to other individuals, whether that be hand washing or going through and making sure that the people that are on enhanced barrier precautions are actually donning and doffing correctly or whatever we have to do for that.
We're able to see who needs to be on hands barrier precautions based on their cultures and sensitivities and everything else. And it's right at our fingertips regardless of where we are. We can be at home looking at this. It can be our floor nurses, it can be the scheduling individual. It doesn't matter. We are able to go on there and see the current up-to-date status of all the infections that are going on in our facilities.
Christina Haeg:
And that's something that you weren't able to do using spreadsheets or paper audit tracking?
Michelle Ehrenberg:
Oh, absolutely not. And if you're not in the building at one point in time, you're emailing or calling or trying to figure out, hey, what's going on? So and so hasn't been feeling well. Have we looked at maybe is this going to be an influenza outbreak? What can we do to combat this outbreak? Is it norovirus? Are we looking at C. Diff? What is going on? And having to go through the chain of we're going to email, we're going to call, we're going to have a Teams meeting instead of just being able to open it up on your computer and see it for yourself.
Christina Haeg:
Yeah, love it. And given your operational background and being the administrator and then also seeing these four communities, what's your involvement in infection management? Most of the time, we hear our nurses saying, it's all on me. I'm the one that has to do all these things. And you've been such a huge advocate for getting your team this extra support and resources with software. What's your involvement in infection management?
Michelle Ehrenberg:
Essentially, when we implemented the software, it takes it off that one person. So you're able to have your charge nurses and your scheduling individuals putting in staff. You're able to have the RN on duty or the charge nurse on duty say, oh, I just got a fax back with their cultures and sensitivities. I'm going to put this into the program. So instead of having one person doing everything, it's a collaborative effort, and then that infection preventionist just gets to oversee the program rather than running the day-to-day through the program. And it really just evens out the workload for everyone in an easy to use format.
Christina Haeg:
Excellent. Which I think is a great segue to our infection preventionist on the call, Angela Mitteness. Angie, you've been a nurse for coming up on 20 years here, and five of those years has been in infection prevention. And you really love understanding why behind this and using data to improve outcomes and being able to educate and audit. And so, can you bring things back to that R.U.G.S. acronym and talk about those four commonly tracked and trended infections and how your life is easier getting things off of spreadsheets with those?
Angela Mitteness:
Right. Yeah, absolutely. So I mean as Michelle alluded to, when you have the spreadsheets and the different Excel programs and all of that out there, it's not easily tracked. You can track it, but it's not pretty much as close to real time as you can, which in working in healthcare, time is very helpful to get on top of things. And when we track if they have anything respiratory going on especially, or any GI, or the UTIs, as I'm using this program, it's easier to be alerted to something quicker. And my staff know too. If they put something in, one of the great things about the program that we're using, Peerlytics, is, it follows McGeer's criteria. So when they're putting this information in, they too can see, was it meeting this, this and this?
So when they kick off that SBAR to the physician, they have everything that they need to say, this is going on, we need something with this. Or they can help monitor it. And then, it also, just through my education and stuff is getting them on the precautions needed. So helping it real time can really help get in control of that, whatever's going on, faster to appropriately treat it or wait and watch or something like that.
Christina Haeg:
Love it. So we know because we're in infection management and in it every day, but I hear all the time about prepping for cold and flu or COVID. And there's so much beyond those respiratory illnesses. What are some of the best practices that you've seen that can lead to a safer cold and flu season in how things are tracked and trended? But then beyond that, norovirus as Michelle had said. What are some best practices that you can share with this group?
Angela Mitteness:
So my big thing and my staff all know it, I'm a big hand hygiene girl. It's the most basic elementary form to help prevent anything. Most of the viruses comes from touching a surface and then you touch your mouth or you touch something or whatever. So I enforce hand hygiene, I reinforce hand hygiene and I promote just making sure that they're doing it adequately. Whenever I get asked and I go to some nurse meetings, I do activities to help them understand the importance of, I have this glow germ stuff and I'll put it on a pen and then I'll have them sign in with their pen and then I have my black light and I go around and I'm like, look at it. This is why hand hygiene is so important, because now, look at we were just touching this one little thing and you guys were going out.
This is the safe zone. It's not going to give you anything terrible, but it's just the visuals. I do all kinds of stuff because that is first and foremost to make sure that you're staying on top of any kind of viral season coming upon us. Also, I mean, I always promote resting well, eating well, drinking, doing all of that, just your self care. You have to do that in healthcare. It is at the utmost importance to take care of yourself so that you can take care of others, because those are the super important things to go kind of above and beyond that. And getting vaccinated, making sure you're current on your immunizations. Doing everything that you can to protect yourself and the people that we care for. We're in the healthcare industry. This is our choice, this is what we choose to do, so we have to do what we can to help protect them.
Christina Haeg:
I love that so much, Angie. And I bet I'm not alone that I just used hand sanitizer on my hands and took a drink of water. So thanks, Michelle. Great reminders. But like you said, the basics but seriously so important. And as you were talking and shared those great tips and tricks, I was just thinking how Michelle had said spreading the workload from her infection preventionist so that her infection preventionist can really just manage all of those pieces. So when you're not the only one entering in this information or tracking and trending symptoms that the residents have and getting labs inputted into different systems that, when you have other people doing that for you, then you're able to put the thought and the education behind the whys for things. And so that was really great. Thank you for sharing that.
Angela Mitteness:
Yeah, absolutely.
Christina Haeg:
Were there any questions you had for the team here?
Mark Anderson:
So a question come in about data. I think for a lot of nurses and clinicians, manual systems are largely used out there. For both of you, when you moved all your systems to a technology-based infection control management practice, what are the data points that you are able to get out of the technology that you just weren't able to get from paper-based systems or an Excel document? What's been kind of the aha moments or the data things that have really helped you do what you want to do with infection control?
Angela Mitteness:
Is it okay if I go, Michelle? I'll speak first. So my background is mostly, for the last probably 17 years, has been hospital based. And so I started in a different regulatory compliance issue with infection control. We had a different computer based system that we used for all of our stuff, so I was really used to that. So I guess the eyeopening part for me was when I came to long-term care, and it was very much, I mean, we were not doing anything that was in the lack of better terms up to date with anything. It was all paper, it was all just spreadsheets and stuff and you would have to go back and forth and the risk of a transcription error from going back into that because it wasn't getting put in right into the system. And so putting stuff right into this Peerlytic system, everything is right in there.
Anything that we would need. That has very much helped make sure that my data is more accurate and I can be more confident that it's accurate too. And then utilizing everybody else who helps put in the data and know nothing gets missed from lack of reports that we might have not been able to pull up before from certain spreadsheets and making sure. So all of those. And then with the Peerlytics, like we can track the infection rates super easy. My automatic stewardship is easier to track because I can do all types of, I do the usage, I can do prescribing the providers, I can do all of that. It's just so much more. I mean, it's all in one, so it's so much more efficient to be able to do it. And having this as well is making sure that I'm meeting all my regulatory compliance issues that we have to have for all of that.
There was a big gap in that when I came in seeing that we had none of that in place, and I mean, there was parts of it in place, but there was some questions of like, well, we need to make sure that we're doing this right. And when you use a system like that, it does that compliance, and I make sure that you're working with it so that you can get all of the data for your copy meetings and all of that that you're working on with your improvement projects for where you need to target things, what you need to look at.
So that part makes the data just easier to access. And when the reports are made too, they're very easy to read. That's huge as well because it's hard to interpret some of the reports when they come up in a certain way from Excel spreadsheets for other people. And when you're trying to educate and work on your quality improvement, the visuals help a lot. It helps to drive that. So that's one really good thing with Peerlytics is those visuals on there. So I rambled a little bit, but it was more.
Mark Anderson:
How about you Michelle?
Michelle Ehrenberg:
Essentially the aha was the real time reports. We have physicians in and out of our buildings all the time, and it's, well, what's going on? Especially when you have a provider that sees 90% of your people and he's going, okay, what's going on? Let me see. And you can run the report without having to go through and make it next [inaudible 00:39:40], making the visuals to bring to QAA and copy and everything else. My medical director will go in there and just look. Our providers can go in there and just look as to what's going on.
They can have, instead of saying, okay, well, here's their point click care login, why don't you go into documents and look under this? They're able to go in there and see, oh wow, okay. All of the SBAR that they've been sending me has been coming through here. It automatically does it for us. It's all right there for us. And then they can look at it in real time and see what's going on, because then they can determine their own patterns or not if that's what they want to do without having to look at the visuals as well.
Mark Anderson:
Yeah, thank you for that. And a lot of us are visual understanders, visual learners. And so, one of the features that I love about the Peerlytics software system is you can put your building diagram in there and then visually color code and track emerging existing and resolving infections. Maybe you guys share a little bit about the experience of that and what that does to help feed your infection control practices. I've not used that, but I've seen it. I can't imagine not having that after seeing it. What's your reaction?
Angela Mitteness:
It's great. And Michelle had spoke to it a little bit before, especially because we use this for employees too. So when it's placed on the map, you put in your information and there's color coordinations on what you can see. But it shows you where the employee worked, when they worked. And then it'll show you two residents that have some type of anything going on with them. So you can literally visually see on the map a cluster of, if something lights up over here, you're going to go to that. Yeah, there it is, Christina. So you can go to it and you can visually see that that's where you're going to focus. We got something going on right here. So it helps to see how, and Peerlytics will pop that all in and it's just an easy, where you can go zone into what you're going to be doing and figure out a plan to get this under control.
Mark Anderson:
That's great. Anything to add to that, Michelle? I mean, I don't know who wouldn't want that after seeing this.
Michelle Ehrenberg:
The only thing that I would add to it is, it's not just staff. We can see with having this lit up, the different color coded everything. There's at times where you can see, okay, well, they're all eating the same thing for dinner, they're all having the same symptoms. You can track where it's coming from more than just the staff. Or they're all having allergies, they're all having runny nose symptoms. Okay, well let's look at, in the library, they've had the door open for the last two days, so now we can figure out why all these people have this. Because it's not just infections and things like that that you track. We can track everything on here for their signs and symptoms. And this with the mapping feature makes it a lot easier than it used to be, taking a highlighter into your facility map and color coding it going forward and trying to do it on paper. It's so much easier.
Mark Anderson:
So we have a great question from a participant today, and they're interested to know, what kind of trends have you been able to see from using the software in managing infection control practices? What kind of trends have you been able to see within the data that's been helpful to you?
Angela Mitteness:
A couple of things stick out in my mind right away for our facilities specifically. Antibiotic usage. I am big on antibiotic stewardship and to see prescribing and criteria used. So watching who's prescribing, I can see who's the big, who is trending doing this when there's not McGeer's Criteria met and for other reasons. I can watch all of that. And then the second one I would have to say would be, well, just tracking the general infections, just to be able to see. And it helps for reports mostly to just see where my clusters have been on my households and stuff. That's been really good. I had it up. I was going to see one more, but I think those are the big ones. Antibiotic stewardship has been really helpful. And then tracking for appropriate criteria met if you're prescribing.
Mark Anderson:
What about you, Michelle? Have you noted any trends in the data that's been interesting or helpful to you?
Michelle Ehrenberg:
So I've had a facility that has been able to combat UTIs. We had issues over and over and over again with people getting UTIs. Why are they getting UTIs? We're doing everything we're supposed to be doing. How is this happening? And we would be able to see, okay, well, this one has symptoms, this one has symptoms. And we were able to stop that and be like, okay, well, we're going to push fluids today. We're going to do this. We're going to do hand washing audits and then be able to essentially stop it before it's a full blown infection and do whatever we can on our end to prevent that from happening. When we were doing it on paper, it was taking us sometimes weeks to be able to see, oh well, there's a pattern. We've had four UTIs on the same end of the hallway in the last six weeks. Oh, we should really do something to make sure this doesn't happen again. But now we can be proactive rather than reactive because we have all of the data right there.
Mark Anderson:
That's awesome. I love that story. Maybe for each of you, I'll just ask, what would you say to the senior living provider who would tell you, we don't need technology to manage infection control? It's not really that much of a priority. How would you guys react to that? You're both smiling, so I know you've got a smart answer.
Angela Mitteness:
Infection control is huge. It is a highly regulated part of what you need to do. I mean, in healthcare, you need to make sure that you're doing everything you can. And infection control isn't just putting on a mask. It's so much more. It's the antibiotic usage, it's the being proactive versus reactive, being able to do that. And when you have a program that you can have multiple people putting this information in and then your infection preventionist can oversee that, infection preventionists, they should not be just sitting behind a screen all the time or a computer entering data. They need to be in interface, out on the floors like watching and helping and doing that. So this allows that time to get out there. You need to be out and about. It should not be just a desk job that you're working at. You need to be visualizing, you need to be educating and you need to be out there auditing, doing all of that. So this very much helps with that time efficient aspect of that so that you can do all of those other parts.
Michelle Ehrenberg:
Mine's a lot simpler. I honestly feel that one of the most damaging sayings you could ever say is, we've always done it this way. Because you've done it on paper forever, you've always done it this way. Well, what have been the results of that? If you always do what you've always done, you're always going to get what you've always got. It's never going to get any better. You're going to be in the same cycle over and over again. So you can certainly try to keep doing it the way you've always done it, but usually there's a better way.
Mark Anderson:
Yeah. So somewhat related to this. So a good question here on keeping all the records straight. So a participant is asking, who inputs all this information into the system so that it's kept up to date. And the concern expressed is that the nurse, the DON, others would actually have more work to do in something maybe in data entry. What's been your experience in other forms of, I guess you could say record keeping for infection control practices versus moving to technology and putting everything in there?
Angela Mitteness:
Well, when it was just the spreadsheet, that was just the infection preventionist or the ADM who was usually managing all of that. I have my nurses, I have my charge nurses, I have everybody who's getting that information, seeing that they put in the information into the system. And so then what I do, when I just go in there, review it, make sure that the outcomes in the 72 hours, but it's way less time because you have multiple people who are out there watching instead of you have to gather all that information from them and you are the only one who puts it in.
Mark Anderson:
Makes it more efficient sounds like. Spreading the work across more people.
Christina Haeg:
Right. Can you hear me Mark?
Mark Anderson:
Have you had an experience with a regulatory compliance surveyor in looking at your infection control practices using the software? Or have you used the software during a compliance survey to help demonstrate compliance? Maybe talk about that. One of our participants has asked.
Angela Mitteness:
Yeah, I'm new to this. It's only been, I've had it since last November or so, and I haven't had our survey yet since I've had it. So Michelle can probably speak to that.
Michelle Ehrenberg:
So essentially, surveyors come in and we just sit them down next to us and say, "Hey, we have this program. Would you like me to print you off the mapping? Want me to print you off the graphs? How would you like to see this information?" And typically they're like, "Hey, that's pretty cool. Can I have a see?" And then typically they end up just sitting down with the surveyor and going through the program and what it has to offer and they're like, yep, you've checked all the boxes. Looks good. And it's not the bring your huge binder and sit down with them and go through each divider, and okay, well, here's all my tracking, here's my trend, here's our antibiotic timeouts. It's really a much seamless process that takes about 15 minutes to go through instead of the typical hour and a half with your three ring binder that is eight inches big.
Mark Anderson:
Awesome. Christina, any final questions? Those are all the questions from participants.
Christina Haeg:
Can you hear me?
Mark Anderson:
Yes.
Christina Haeg:
Okay, excellent. I am at a work retreat and so I apologize for my poor internet and lack of what appears to maybe be engagement here, but this has been so, so fantastic and I love hearing all of these real world use cases and hearing your lady's expertise in this topic. And to kind of follow up to a question that was asked about fearful of adding more work to someone's plate, I think the big thing that we've heard from our clients is, it's work they're already doing. It's just either being done inefficiently, it's being done disjointed in several different ways by several different people. So this just allows things to be a lot more streamlined and find a succinct workflow that can spread that workload. So this has been really great. Thank you everyone.
Mark Anderson:
Well, thank you Christina. And I want to thank our guests, Angie Mitteness and Michelle Ehrenberg for sharing your experience and your expertise and your thought leadership on this topic of infection control management, but also in how technology has helped you achieve your goals and serve your needs in those areas in your work. So thank you for good work with that. Thanks again, Christina, for being a part of this webinar series. Really appreciate it. And we'll have to bring you guys back again sometime. I want to also let our participants know, our next regularly scheduled leadership forum webinar is July 12th. We're not doing it the first Wednesday of the month because of the 4th of July holiday.
And I'm just thinking there might be too many people away out at the cabin or doing something else at that time. So we are going to move that to the next Wednesday. For this webinar series and any of our other webinars, you can go to eldermark.com. The webinar's link is on the website and you can sign up for this series or any other webinars that we offer to our customers here at Eldermark. Thanks again to Christina, to Angie, to Michelle. Really, really appreciate your presence here today. And thank you again for your good work. We'll see all of you participants hopefully again next month. Thanks for joining us today. Really appreciate it. Take care.
Get Awesome Senior Living Content Delivered Straight to Your Inbox!
Posts by topic



