

California didn't just add paperwork this year. It changed what counts as proof.
A resident has a fall. A change in mood. A new struggle getting dressed. Under Title 22, that's a significant change, and it triggers its own reappraisal, on the spot, not whenever the next annual review happens to land. Before that reappraisal is finalized, someone has to reach the resident's physician, and the contact, what the physician said, and what changed in the care plan all have to be on record. Every resident gets an annual medical visit now too, documented as done or documented as refused. And when your team writes up a behavioral change, the write-up has to show the condition, who got involved, the care plan, and that you tried the least restrictive option first.
None of that is a future problem. Multiple compliance groups are already calling 2026 the first year CCLD is actually citing against it, not just warning about it. If your last reappraisal is sitting in someone's memory instead of on a timestamp, that's the gap a surveyor finds first.
The Space Between “Something Changed” and “Someone Noticed” Is Where Citations Start
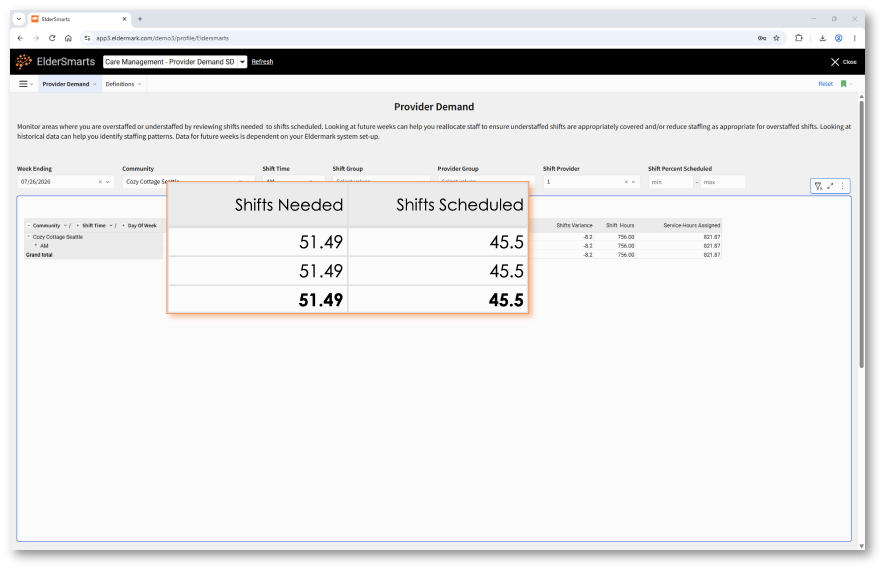
A resident's needs shift faster than a fixed schedule can catch. Staffing gets built around what a caregiver assumes, not what a resident actually needs that week. That mismatch is exactly what surveyors are trained to find: care that doesn't match what's documented, reappraisals that lag behind reality.
Eldermark ties your staffing to real-time acuity, so when a resident's needs change, the gap between “needed” and “scheduled” shows up on your screen before it shows up in a survey finding.
Every Caregiver, Every Resident, the Same Standard
California's dementia-aware standard doesn't stop at your memory care wing anymore. Any resident, diagnosed or not, who shows a cognitive or behavioral change now has to get the same level of attention and the same quality of documentation. That only works if every caregiver is writing things down the same way.
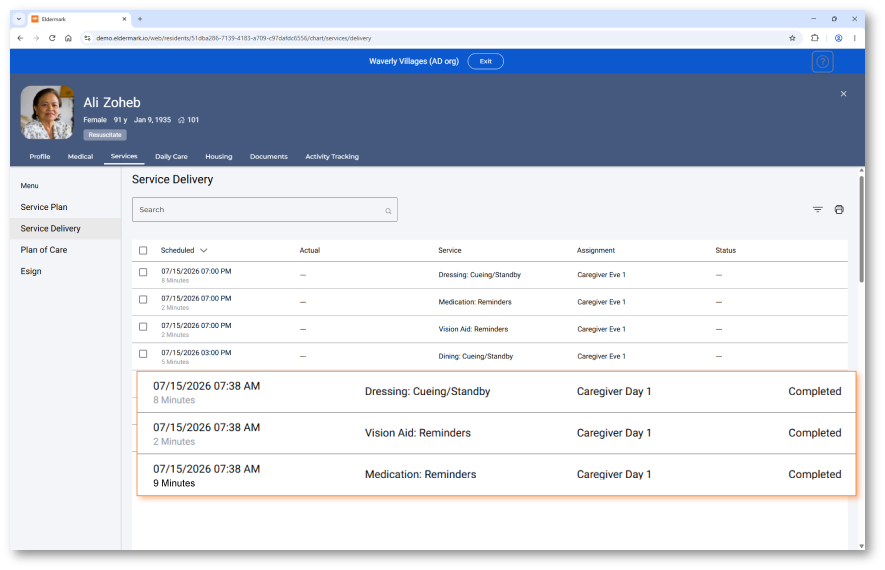
Eldermark turns a caregiver's observation into a structured, standardized record: same categories, same format, every resident, every Community. When a behavioral change gets logged, the condition, the professional involvement, and the care plan are already sitting in the same place, not scattered across a caregiver's notes and someone's memory of what happened that shift.
Physician Contact. Care Plan Change. Timestamped, Not Reconstructed.
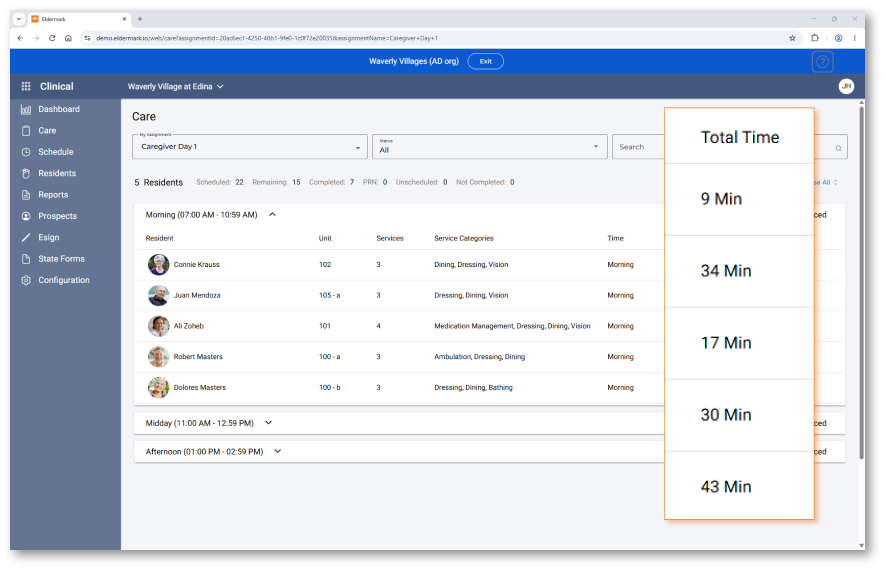
The hardest part of Section 87463 isn't doing the work. It's proving you did it when someone asks three weeks later. Who called the physician. What they said. What changed in the plan because of it.
Eldermark logs all of it automatically, as part of the workflow your Clinical Leaders are already using: who made the change, when, and what it was before and after. Nothing extra to fill out after the fact. Nothing to piece together from memory when the survey letter shows up.
Don't Wait for a Citation to Find Out Where the Gap Is
See how Eldermark connects acuity, care delivery, and reappraisal documentation into one record you can actually hand a surveyor.
Talk to EldermarkFrequently Asked Questions
A package of updates to Title 22, Division 6, Chapter 8 took effect January 1, 2025, covering RCFEs specifically. It expanded dementia-aware care standards facility-wide, rewrote Section 87463 to require reappraisals whenever a resident has a significant change (not just annually), expanded the annual medical visit requirement to all residents, and raised the documentation standard for behavioral changes.
The regulation defines it broadly: a fall, a stroke, a new decision-making impairment, or any meaningful shift in a resident's physical, cognitive, behavioral, or functional condition. Each one triggers its own reappraisal, separate from the standard 12-month review.
Yes. Before finalizing a reappraisal, the facility has to contact the resident's physician or specialists and document that contact, what was recommended, and any resulting care plan changes.
It's active. The rules took effect in 2025, but multiple compliance consultancies point to 2026 as the first full year of aggressive, statewide enforcement, meaning facilities are already receiving deficiencies and corrective action plans tied to these standards.