What Is an eMAR? — A Complete Guide for Assisted Living Operators
Medication management in assisted living is harder than it looks on paper.
"I can't be on the floor 24/7. I need to know when a med pass is late without physically walking the building."
Every clinical leader reading this has heard some version of that sentence. In assisted living, medication management is a visibility problem, a workflow problem, and a compliance problem. The right eMAR solves all three.

What is an eMAR?
An eMAR, or electronic medication administration record, is the digital system used to schedule, document, and track medication administration. It gives your team a live, consistent record of what medications are due, when they are due, and what happened during the med pass.
In assisted living, the right eMAR does more than replace paper. It helps staff manage med pass more consistently, creates a clearer record of what happened, and gives clinical leadership better visibility into medication activity across the building.
The real question is not just what an eMAR is — it is what happens in your building without one. In assisted living, medication management is not just a documentation problem. It is a visibility problem, a workflow problem, a compliance problem, and often a communication problem between care staff, pharmacy, and clinical leadership.


Why eMAR matters in assisted living
Medication management in assisted living is harder than generic healthcare content usually makes it sound. Residents are moving in later. Acuity is rising. Medication lists are longer. Orders are more complex.
A single med pass may involve routine medications, PRNs, vitals-based parameters, time-sensitive administration windows, refill coordination, and psychotropic documentation expectations. Executing that consistently requires a structured administration framework and accountability at every step. On top of that, many communities rely on med techs to carry out medication workflows that still require consistency, accuracy, and accountability. That is a difficult system to run well on paper.
The best assisted living eMAR systems help staff follow the right process in the moment, help clinical leaders see what is happening without walking the building, and help communities stay audit-ready without digging through stacks of paper after the fact.
For assisted living communities, eMAR is not just a technology upgrade. It is an operating system for one of the most risk-sensitive parts of the building.
How does an eMAR work?
A caregiver logs in and sees what medications are due for each resident — schedule, administration details, and any related instructions. As the med pass happens, the caregiver documents in real time, along with any refusal, delay, omission, or required follow-up. That creates a live, time-stamped record tied to the person who completed the task.
Workflow that guides care in the moment
A paper MAR can show a medication was due. It cannot guide the staff member through the process consistently, provide surface-level visibility across shifts, or help a clinical leader see what is happening community-wide without manually reviewing charts.
Documentation that clarifies the next step
When documentation is clean, time-stamped, and centralized, staff can see what was completed, what still needs attention, and what changed since the previous shift. That reduces the friction that builds when handwritten notes and disconnected systems carry too much of the workload.
Medication education standards →Visibility without walking the floor
An eMAR helps clinical leadership answer questions faster: Was the medication administered? Was it late? Was it refused? Is a refill needed? Is this an isolated issue or a broader pattern? That visibility changes how quickly a team can respond and how confidently a clinical leader can stand behind the documentation.
What is medication reconciliation →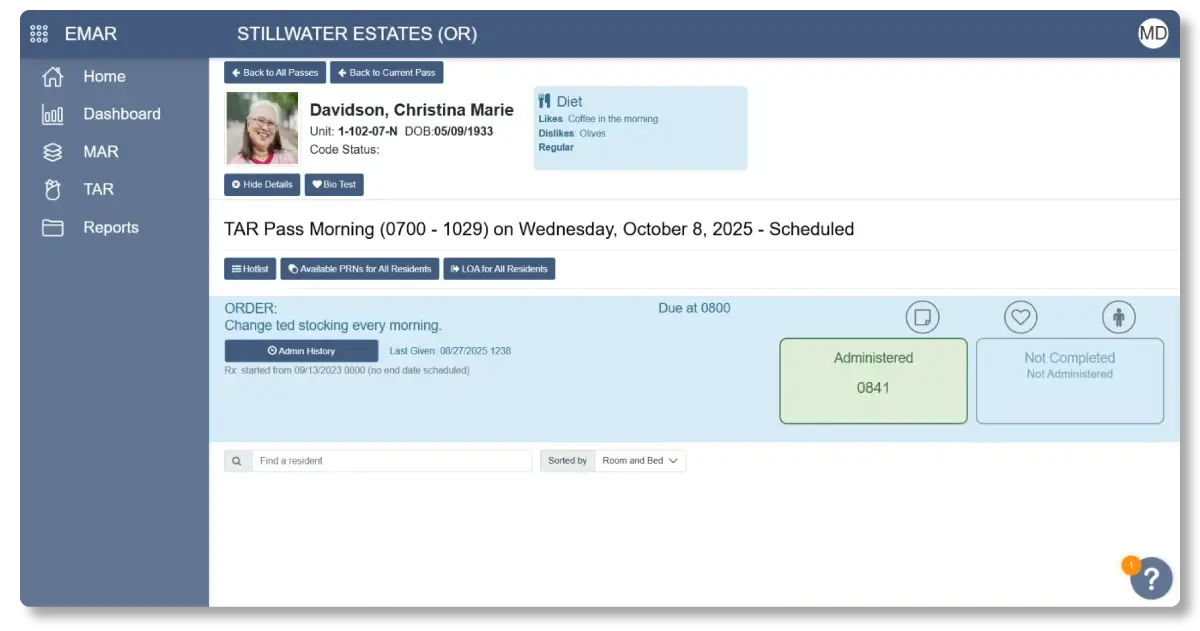
eMAR and compliance: why survey readiness matters
"It collects data and allows us to easily see trends and capture areas we can focus on quality improvement."
Kayla G.
That is not just a convenience issue. It is a compliance issue.
Assisted living is state-regulated, and medication administration documentation remains one of the clearest places where communities have to demonstrate consistency and control. The medication safety officer role is central to that process, and eMAR is one of the primary tools that role depends on. When the documentation trail is messy, incomplete, or difficult to retrieve, the risk is not just operational — it becomes regulatory.
Paper MAR slows retrieval. It introduces interpretation problems. It leaves too much room for the record to appear finished when the workflow behind it was not.

Survey-ready documentation should be:
That is what an eMAR supports. That is what paper cannot consistently deliver at the level of complexity assisted living communities are now carrying.
Why integration matters more than features
A lot of buyers get pulled into feature comparisons too early. But in assisted living, the larger issue is often architecture.
A standalone eMAR may remove paper, but it can still leave your team doing the integration work manually. Medications in one place, care plans in another, pharmacy communication somewhere else. The building still operates through handoffs — it just does so digitally. That is not the same thing as a connected workflow.
An integrated eMAR changes what your clinical team can actually see and do:
That is the difference between a system that documents med pass and a system that helps the building run better.

The case for eMAR: what clinical leaders need to know
The clinical leader who needs to make the case for eMAR usually has a stronger argument than they think. This is not a quality-of-life purchase for the care team in isolation. It is a building-level clinical decision with direct implications for risk, compliance, and the capacity of your team to do their jobs well.
The four dimensions below are where the argument is clearest — and where the cost of staying on paper is most visible.

Medication workflows carry too much consequence for a fragile system
A community without real-time visibility, a strong documentation trail, and cleaner staff guidance is carrying more clinical risk than it needs to. When something goes wrong, the documentation is the first thing a surveyor asks for.
What is a drug utilization review →Survey readiness becomes fragile when documentation is hard to trust
When documentation is hard to retrieve, hard to trust, or hard to interpret, survey readiness becomes much more fragile. eMAR strengthens the trail when the building needs to demonstrate what happened, when it happened, and who was responsible.
Time on paper is time taken away from residents
Time spent on paper reconciliation, duplicate documentation, and manual follow-up is time taken away from resident care. The more efficient the medication workflow becomes, the more clinical capacity your team gets back every day.
Disconnected workflows create preventable problems at every handoff
A disconnected medication workflow creates preventable problems between care staff, pharmacy, and clinical leadership. A shared, accurate record reduces that friction at every handoff point.
Read the case study →